0
£0.00
0 items
Diagnostic ultrasound is technically challenging and has a steep learning curve. Adapting techniques to accommodate technical issues and patient presentation to generate consistent diagnostic images can be challenging, as is the interpretation of subsequent images to arrive at a well-reasoned, differential diagnosis (Smith et al, 2015).
Despite its undeniable value in a wide range of musculoskeletal conditions, several issues regarding training and competency are still to be addressed. There is no standardised training curriculum, there is a lack of recognised training programmes and very few adequately trained and willing clinical supervisors. These are significant obstacles to the more widespread use and future of musculoskeletal ultrasound (Taggart et al., 2006).
As an unregulated imaging modality, diagnostic ultrasound can be used without formal training. The term 'sonographer' is not regulated and can be added to a clinician's professional title i.e. it is not a protected title.
Although the procedure itself has no specific side effects, harm may result from incorrect acquisition and interpretation of images owing to operator inexperience and/or poor equipment.
We must be aware of the pitfalls and limitations of ultrasound, our own competency/experience, and the medico-legal implications of carrying out a scan. This is particularly the case for relative beginners and those working in isolated non-supportive environments for example solo-practitioners in private practice. For beginners from the outset, we advise clinicians keep a log book of their scans and audit their own practice (Taggart et al., 2006).
Current education and training for both medical and non-medical ultrasound practitioners lacks standardisation. Despite the increasing use of musculoskeletal US there is no consensus yet regarding the standards required to achieve a basic level of competency in the use of this imaging technique. Recognition of ultrasound as a speciality may help to expedite national guidelines. This would also prove important from a clinical governance perspective, however such a speciality would appear to be a long way away.
Starting out?
At SMUG we believe all clinicians should strive to achieve a basic level of competency in MSK Ultrasound (whatever your profession). This is one of the reasons we set up our SMUG Mentorship Programme, to provide a learning pathway to achieve this competence. Adequate training and recognising one's scope of practice lies at the heart of the competency debate. It is the responsibility of the clinician to provide evidence of their learning and clinical reflection.
Courses can be divided into 1) non-competency based (attendance only) and 2) competency-based courses.
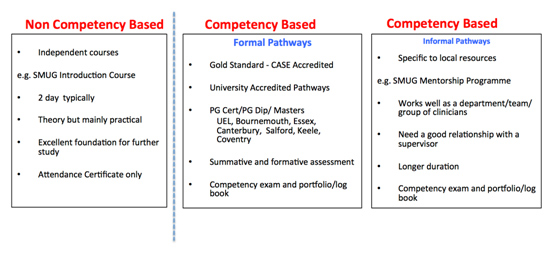
(1) Non-competency based courses (often known as 'short courses')
Short Courses:
Introductory short courses (normally 2 days) provide an excellent introduction for those who want to get started in MSK ultrasound imaging or develop their basic skills. Our SMUG 2-day Introduction to MSK Ultrasound Imaging in Sports Medicine course is accredited by the Royal College of Radiologists (RCR), Faculty of Sports & Exercise Medicine (FSEM), and the European Society of Musculoskeletal Radiology (ESSR) and is a very popular course with a variety of clinicians (Introduction to MSK Ultrasound). The Introduction course is a highly practical 2-day course with a high machine to student ratio and expert tutors for close supervision and feedback - ideal for learning MSK ultrasound imaging.



(2) Competency based courses
Competency based courses vary from 'formal learning pathways' such as PG Certs, Dips and MSc's to more 'informal learning pathways' such as the SMUG Mentorship programme. The goal is to gain, and be able to prove, your competency via a structured pathway with summative and formative assessments. Competency is a very grey area, particularly as there are so many ways that ultrasound is now being used. It is used in a variety of ways by different professions, and so 'competency' is specific to how you will be using ultrasound in your clinical practice. Over the years our delegates have had many different reasons for attending our courses - here are a few:
a) A shoulder surgeon attended our course to be able to differentiate full thickness tears of the rotator cuff from a tendinopathy without sending the patient for an MRI, as this determines the client's pathway.
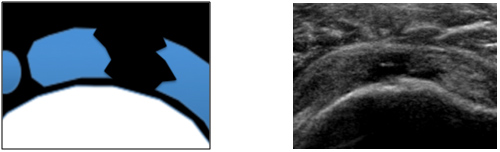
Figure 1: Full thickness tear of supraspinatus in transverse section
b) A physiotherapist who works at a Premiership football club wanted to use ultrasound to help guide rehabilitation following muscles tears particularly the calf and hamstring tears.
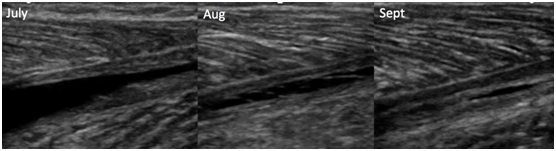
Figure 2: Aponeurotic tear of the medial calf - serial scans from July to Sept to demonstrate healing and help guide rehabilitation
c) A hip consultant attended the Introduction and Cadaveric Injection course to be able to assess for a hip joint effusion, to avoid the requirement of an MRI and to guide his hip joint injections using ultrasound instead of taking them into theatre.
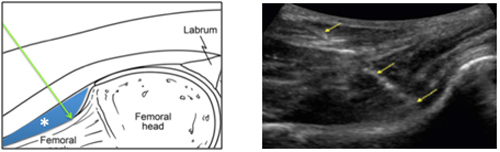
Figure 3: Technique for an ultrasound guided intra-articular hip injection - longitudinal in-plane approach
There are many more examples but this highlights how competency is specific to how the clinician wants to use ultrasound in their clinical practice. So, any competency framework or guidelines must reflect this and be flexible enough to allow clinicians to prove their competency for their specific role.
As a result, (The Royal College of Radiologists (RCR) and the (Faculty of Sports and Exercise Medicine (FSEM) advocate a 'modular' based competency pathway. A 'module' can consist of a joint or area e.g. the shoulder or ankle, or it could relate to a specific intervention e.g. a guided hip injection.
MSK ultrasound lends itself very well to this approach and so gaining competency will mean different things to different clinicians and will require a different learning pathway. It is important to note that some modules or joints will take longer than others to gain clinical competency. For example, if a clinician wants to learn how to scan the Achilles and patella tendon this can be achieved relatively quickly, however to be able to scan the shoulder and be able to differentiate a partial thickness from a full thickness rotator cuff tear will take longer. The shoulder is a more challenging area and will require a longer learning pathway and more dedicated teaching, supervision and practise.
The requirements to gain competency will also vary according to your specific professional guidelines, for example the Royal College of Radiologists (RCR), the Faculty of Sports and Exercise Medicine (FSEM) and Society of Radiographers (SOR) have produced guidelines on how to achieve competency in MSK ultrasound. Unfortunately, physiotherapists, GPsWI, Osteopaths and Chiropractors will struggle to find specific guidance from their respective bodies. I would advise these professions read the RCR guidelines.
Whatever your clinical background and your ultrasound goals there are elements that must be fulfilled to prove competency in MSK ultrasound. These are:
- Attend the appropriate courses
- Spend time observing and scanning with a variety of clinicians from different clinical backgrounds
- Gain direct experience and supervision with a suitably trained clinical tutor/supervisor
- Keep a logbook of scans
- Audit your scans and reflect on the results/discrepancies
- Pass a competency-based exam
This should be a continual cycle of learning, reflecting and developing your skills.
Formal Learning Pathways: The Consortium for the Accreditation of Sonographic Education (CASE) approve postgraduate university-based courses and are advocated by professional bodies such as the British Medical Ultrasound Society (BMUS) so that trainees can learn and demonstrate their competency in areas such as ultrasound physics, safety, anatomy and pathology-specific knowledge. However, gaining competency in effective scanning technique and differential diagnosis presents a significant challenge and this restricts the availability of training opportunities (Smith et al., 2015).
At SMUG we encourage clinicians to attend these CASE accredited postgraduate university-based courses (CASE accredited courses). Unfortunately these courses are not a viable option for all clinicians, and there are many barriers to attending them (Figure 4).
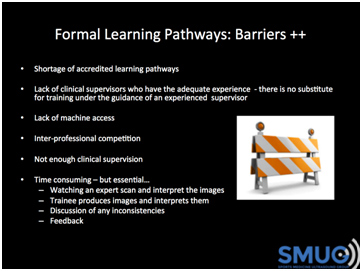
Figure 4: Barriers to CASE accredited postgraduate courses and US training
The main barrier is the lack of adequately trained and experienced clinical supervisors. A significant number of clinicians cannot attend such courses, or they do but cannot get the adequate support and supervision from the supervisor to achieve all elements of the course.
From experience, as a visiting university lecturer and clinical supervisor, it is important to understand that CASE accredited pathways do not guarantee high standards and it is the responsibility of the clinician to ensure they achieve a positive learning experience, adequate supervision, and continue their learning after the course.
Informal Learning Pathways: With the exception of CASE accredited ultrasound courses, there is distinct shortage of accredited learning pathways to gain a basic level of competency in MSK ultrasound imaging. This is one of the reasons we set up the SMUG Mentorship Programme, which is a unique competency-based course which takes place over approximately 8 months with monthly teaching days focussing on different module/joint (Figure 5).
At the end of the course delegates must produce a log book and pass the competency exam.
This is a unique learning pathway and provides a good way of gaining a basic level of competency in MSK ultrasound. It provides a solid foundation for delegates to further develop their scanning skills and their clinical interpretation. Each delegate is appointed a supervisor/ mentor who can also act as clinical supervisor on a CASE accredited university postgraduate course. Delegates this year have been from the UK, Ireland, Norway and Canada.
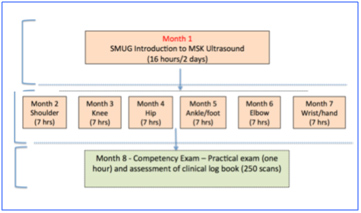
Figure 5: SMUG Mentorship Programme
Gaining clinical competency can be a challenge and often relies on the motivation, finances and commitment from the clinician to seek opportunities that can complement their pathway and are devising informal means of training in order to acquire the appropriate ultrasound skills.
For example, a group of rheumatologists in Belfast published their informal pathway to gaining MSK ultrasound competency over a 5-year period (Taggart et al., 2005). Their experience shows what can be achieved without following a formal learning pathway. However, this route is less structured and relies fully on the organisation, discipline and motivation of the individual. In a recent departmental audit, they estimated that US scanning influenced the clinical management of their patients in 70% of cases.
Such pathways take many years and although they are largely informal, they are in many ways more rigorous and comprehensive than training undertaken by many MSK ultrasound/radiology trainees including those that attend CASE accredited postgraduate learning pathways.
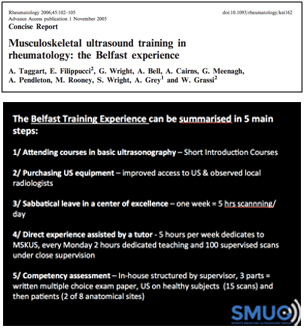
Figure 6: The Belfast Training Experience - how one group of rheumatologists defined and achieved competency
As the leading provider of MSK ultrasound courses, we are passionate about helping clinicians achieve the knowledge and skills required to use MSK ultrasound to further their clinical practice.
For further information please do not hesitate to contact us at info@ultrasoundtraining.co.uk.